
Surgical landmarks of facial nerve pdf
Facial nerve paralysis is a daunting potential complication of parotid surgery and is widely reported. Knowledge of the key landmarks of the facial nerve trunk is essential for safe and effective surgical intervention in the region of the parotid gland.
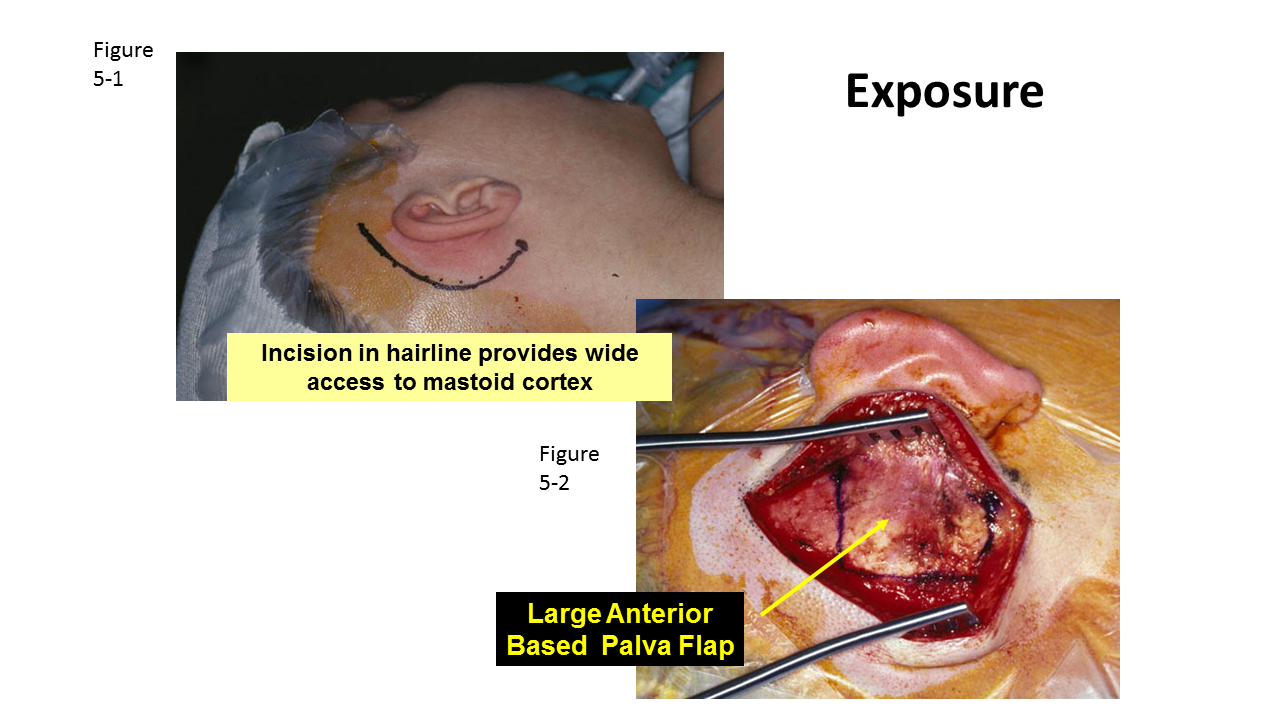
Background: The identification of the facial nerve can be difficult in a bloody operative field or by an incision that limits exposure; hence anatomic al landmarks and adequate operative exposure can aid such identification and preservation.
skeletonization of the facial nerve along the mastoid segment to lower the posterior canal wall to the facial nerve (still covered by bone). The mastoid area behind the facial nerve is later obliterated with a muscle flap to keep the volume of the final cavity low and avoid discharging ears. The other method of “canal wall down” mastoidectomy is front-to-back mastoidec-tomy. Surgeons may
Marginal mandibular branch of facial nerve Mid-inguinal point – half way between ASIS and pubis – landmark for femoral artery in groin. (see lower limb pulses and cardiovascular examination). 18. Midpoint of inguinal ligament – Half way between ASIS and pubic tubercle – landmark for deep inguinal ring and indirect inguinal hernia. Medial to this for direct inguinal hernia. 19. Inguinal
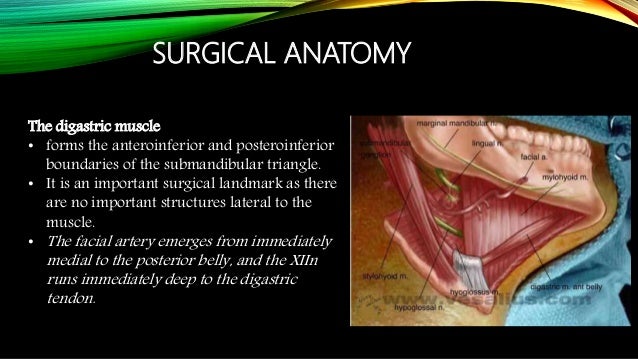
described the facial nerve line, which extends from the lateral surface of the posterior belly of the digastric muscle to the lateral surface of the ascending ramus. 2 The spatial relation-
branches of the facial nerve are frequently encountered during such surgical pro- cedures and are occasionally damaged which leads to an ugly cosmetic deformity due to paralysis of the muscles of facial expression which control the lower lip and corner
Anatomy of Meckel’s Cave and the Trigeminal ganglion
https://youtube.com/watch?v=jnonLwxW2Cg
Facial nerve ppt roger original slideshare.net
Penetration of the parotid gland near the facial nerve has always raised concerns among surgeons because facial nerve injury is an important cause of morbidity associated with parotid gland surgery. The conventional approach is anterograde parotidectomy, in which the main trunk of the facial nerve (facial nerve trunk, FNT) is identified and
24/07/2013 · Aims and Objectives. The aim of the cadaveric dissection was to dissect all the landmarks of facial nerve that has been described in the literature and study their respective anatomical relationship with the facial nerve.
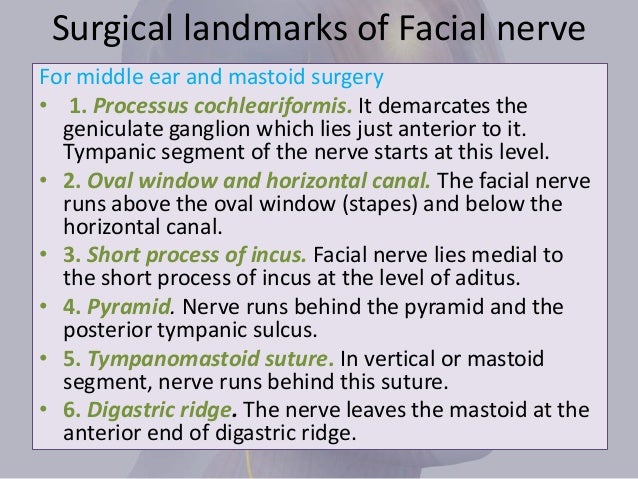
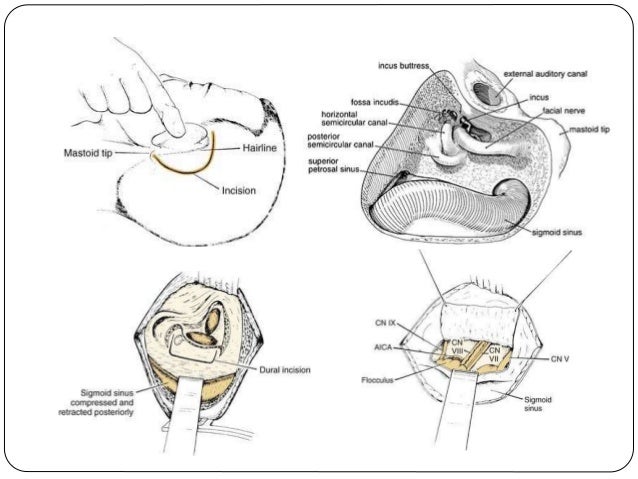
Critical surgical landmarks for this procedure are the digastric ridge (i.e. a ridge of bone, which is posterior to the facial nerve and medial to the tip of the mastoid), the fossa incudis and
A review of the tragal pointer: anatomy and its importance as a landmark in surgical procedures llary artery to the tragal pointer, Frankfort hori- zontal plane, and tip of the condyle (Table 3).
surgery is between 3% and 5% and that of postoperative transient facial nerve dysfunction, between 8.2% and 65% (Witt, 1998). During parotid gland surgery, preservation of the facial
Injury to the marginal mandibular branch of the facial nerve (MMN) during surgery often results in poor functional and cosmetic outcomes. A line two finger breadths or 2 cm inferior to the border of the mandible is commonly used in planning neck incisions to avoid injury to the MMN. The purpose was to compare the two finger breadth/2 cm landmarks in predicting MMN course, and their accuracy
Surgical exposure of the facial nerve.11 Learning to use this landmark requires more surgical expertise and does not predict more accurately the position of the facial nerve trunk than other methods reported. Acta Otolaryngol Suppl. 13. 4.80:261-273.40 (0.03.
Facial nerve paralysis is a daunting potential complication of parotid surgery and is widely reported. Knowledge of the key landmarks of the facial nerve trunk is essential for safe and effective surgical intervention in the region of the parotid
Although the surgical anatomy of the facial nerve has been well documented, the concept of surgical treatment for parotid tumors, facial palsy (neurorraphy techniques) and submandibular surgical approach are rarely challenged now.
In our study, the facial nerve was an average of 5.22 mm from the petrous ridge. The longest distance was 10.1 mm. When drilling at the The longest distance was 10.1 mm. When drilling at the internal acoustic opening of the IAM, one should be cautious until the facial nerve is found.
facial nerve trunk was 3.5 mm (cadaver) and 3.87 mm (live surgery), the tragal pointer was found to be at a mean distance of 16.61 mm (cadaver) and 16.36 mm (live sur-
midface augmentation, alloplastic facial implants, safe zone, infraorbital nerve, anatomic landmarks, nerve block, paresthesia Midface augmentation with alloplastic implants is a common cosmetic procedure; approximately 8800 cheek implant procedures were performed in 2009. 1 It can also be used as an adjunct to orthognathic and reconstructive surgery.
IrJNS. 2017;2(4) 77. surgical landmarks to perform a safe surgery [11]. Due to the stressful nature of the surgery and possible facial nerve injury and so many problems of facial nerve and subsequent
Facial Nerve Parotid Landmark – Free download as PDF File (.pdf), Text File (.txt) or read online for free. Landmarks of the Facial Nerve as it leaves the Parotid Landmarks of the Facial Nerve as it leaves the Parotid
Facial nerve paralysis is a daunting potential complication of parotid surgery and is widely reported. Knowledge of the key landmarks of the facial nerve trunk is essential for safe and effective
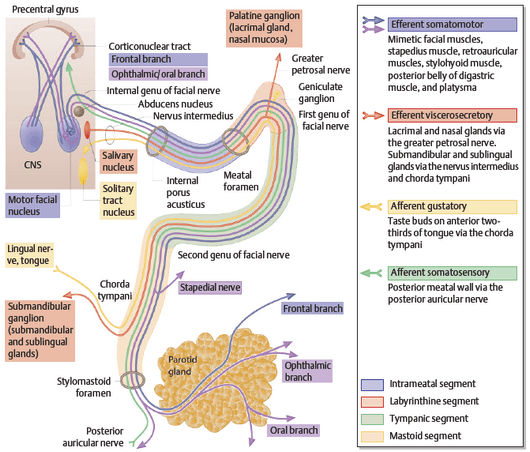
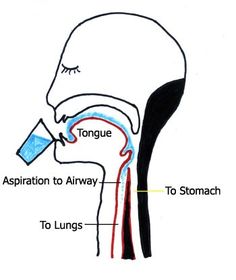
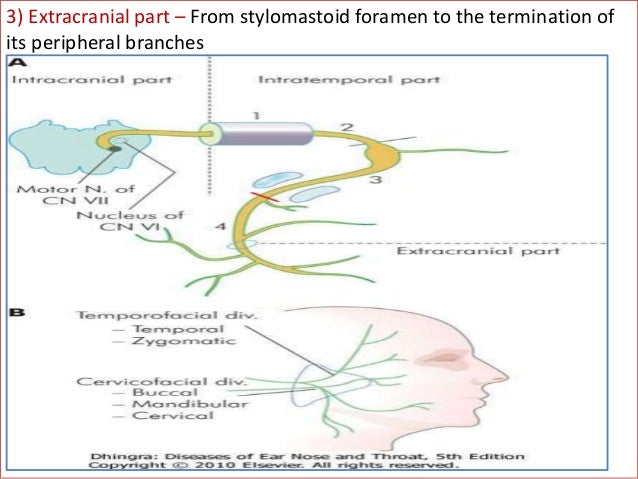
The facial nerve is the seventh cranial nerve, or simply CN VII. It emerges from the pons of the brainstem, controls the muscles of facial expression, and functions in the conveyance of taste sensations from the anterior two-thirds of the tongue. The nerves typically travels from the pons through the facial canal in the temporal bone and exits the skull at the stylomastoid foramen. It arises
Parotidectomy Overview Periprocedural Care Technique
In a parotid surgery, the greater auricular nerve was detected; then the greater auricular nerve and facial nerve diameter were measured by the compass with precision of 0.1 millimeter and recorded. After facial nerve exploration, if the other landmarks of vascular and tail signs are detected, they are recorded in the files.
Facial nerve is the seventh cranial nerve, which supplies the muscles of the facial expression, sensory supply to the an- terior two thirds of the tongue and secretomotor supply to
ANATOMIC BASES OF MEDICAL, RADIOLOGICAL AND SURGICAL TECHNIQUES N. Pather Æ M. Osman Landmarks of the facial nerve: implications for parotidectomy
distance from the arcuate eminence, the facial nerve hiatus, and the foramen spinosum to MC was 16.6, 12.8 and 7.46 mm respectively. The TG The TG lay 5.81 mm posterior to the foramen ovale.
Abstract. Facial nerve paralysis is a daunting potential complication of parotid surgery and is widely reported. Knowledge of the key landmarks of the facial nerve trunk is essential for safe and effective surgical intervention in the region of the parotid gland.
Identification of the facial nerve trunk is essential during surgery of the parotid gland. Numerous landmarks have been researched and used. The relation between the facial nerve to two constant bony landmarks, the tip of the mastoid process and the central point of the transverse process of the atlas was investigated.
Bony landmarks as an aid for intraoperative facial nerve
Division of Plastic and Reconstructive Surgery, Washington University School of Medicine, Suite 17424, East Pavilion, Box 8238, One Barnes-Jewish Hospital Plaza, Saint Louis, MO 63110, USA. Treatment of facial nerve injuries depends upon a detailed understanding of its anatomic course, accurate clinical examination, and timely and appropriate diagnostic studies.
facial skin and Superficial Muscular Aponeurotic System (SMAS) during facial rejuvenation procedures. The aim of this study was to The aim of this study was to define the location of the true retaining ligaments of the face and to discuss their usability as surgical landmarks.
of information on the deep attachments in the cheek.18,21 Recently, studies have begun to in-vestigate deep attachments found in the tem-poral12,25 and periorbital regions.26,27 These ar-
Original Article Surgical Dissection of the Facial nerve in Parotidectomy: Our Personal Experience *Nematollah Mokhtari Amir Majdi1, Mojgan Pourhamzeh2 Abstract Introduction: Salivary gland tumors are relatively rare and constitute 3-4% of all head and neck neoplasms. The majority (70%) of salivary gland tumors arise in the parotid gland. Recommended treatment for a parotid mass is surgical
THE FACIAL NERVE IN PAROTID SURGERY Oliver H. Beahrs, M.D. and Bernard F. L’Esperance,M.D., Rochester,Minn. s=bThe excision of small parts of the parotid gland is liable toresult in damage the facial nerve, which runs through the substance of the gland. Such dam-age is hard to avoid if the nerve is not well exposed, and the surgeon has to choose between the danger of facial …
Surgical management of iatrogenic facial nerve injuries J. DOUGlAS GREEN, JR., MD. CLOUGH SHELTON. cholesteatoma, and revision surgery where landmarks have changed may all contribute to an iatrogenic injury of the facial nerve. The importance of adequate preoperative counseling of the patient and family for the potential for facial nerve injury cannot be overstated. Most otologic …
facial nerve is not a true anatomic separation into two distinct and discrete lobes.1 During parotidectomy, several anatomical landmarks may be used to locate the facial nerve. One of the most commonly employed is the tragal pointer.
Facial nerve palsy is a known risk associated with parotid surgery. Inadvertent damage to the nerve can result in permanent or transient paralysis, corneal irritation from lack of motor function, Frey syndrome, pain, or changes in facial appearance. 1 Common anatomic landmarks that can indicate the position of the main trunk of the facial nerve
– Facial nerve – Facial retaining ligaments Techniques – SMAS lift – Deep-plane lift – Composite lift – Subperiosteal lift Nasolabial fold Non-surgical facelift . Anatomy Platysma muscle – from the lower cheek to the level of the second rib – Three variations of the anterior boarders of the right and left platysma muscle Type1: separated in the suprahyoid region and interlacing
well-defined surgical landmarks, and not at least, the personal experience of the surgeon in this type of surgery. The main roles of monitoring the facial nerve are: reducing the risck of iatrogenic trauma during dissection, mapping the course of the nerve, early nerve identification and warning the surgeon about the proximity of the nerve during dissection (18). Usually there are four
Preserving the marginal mandibular branch of the facial

World Journal of Surgical Oncology BioMed Central
https://youtube.com/watch?v=SSPTV0g3p4Q
Various surgical landmarks of the facial nerve have been investigated to allow for a safer and quicker parotidectomy or other surgery in the lateral face. Surface landmarks for the facial nerve trunk have been proposed. Pather and Osman [14] suggested the use of the transverse process of the axis as the landmark for the facial nerve trunk because it was easily palpated, did not require a
Local Anesthesia Techniques in Oral and Maxillofacial Surgery Sean M. Healy, D.D.S. Oral and Maxillofacial Surgery Francis B. Quinn, M.D., FACS
21/07/2015 · The facial nerve, or cranial nerve (CN) VII, is the nerve of facial expression. The pathways of the facial nerve are variable, and knowledge of the key intratemporal and extratemporal landmarks is essential for accurate physical diagnosis and safe and effective surgical intervention in …
Background. The identification of the facial nerve can be difficult in a bloody operative field or by an incision that limits exposure; hence anatomical landmarks and adequate operative exposure can aid such identification and preservation.
ultrasound anatomy of the facial danger zones robert bard, md director, the biofoundation for angiogenesis research, ny j. pozner, md & l. bass, md plastic surgery center, ny ximena wortsman, md radiologist santiago, chile . imaging parameters linear array 14-18 mhz 3d array 15-17 mhz with surface rendering display linear electronic array 20-40 mhz doppler color, power, spectral with vessel
Errors in facial nerve surgery 319 An example is that of playing chess. A novice may have only a handful of memorized defense strategies.
Daniel Jose C. Mendoza MD Intraoperative Distance Between
Surgical Management of Iatrogenic Facial Nerve Injuries
Background The identification of the facial nerve can be difficult in a bloody operative field or by an incision that limits exposure; hence anatomical landmarks and adequate operative exposure can aid such identification and preservation. In this
Landmarks used to localise the marginal mandibular branch of the facial nerve (MMN) included: the angle of the mandible, facial artery, inferior border of mandible, parotid edge, lobule, gonion, retromandibular vein and massteric tuberosity of the mandible [21,22,23,24].
Facial nerve injury during rhytidectomy is a rare but dreaded complication. Of the various divisions of the facial nerve, injury to the marginal mandibular nerve (MMN) is of great concern in planning for a lower face- or necklift.
variations of the tympanomastoid segment of the facial nerve in relation to fixed known anatomical landmarks in cadaveric temporal bone dissection. 395 . 396 Safer Ear Surgery: Anatomical Study of Landmarks Materials and Methods 35 human temporal bones (18 right and 17 left) were obtained and dissected with standard otologic instruments under magnification using Karl Kaps (Germany) …
⭐⭐⭐The tympanomastoid suture line⭐⭐⭐ ⭐⭐⭐The posterior digastric muscle⭐⭐⭐ The tragal pointer refers to the tragus cartilage, which “points” to the location of the nerve one centimeter anterior, inferior, and deep to the cartilage.
In this particular case, the knowledge of surgical anatomy of the facial nerve and its correlations with the parotid gland is very important for an adequate preservation in the cases of surgery of benign and malignant diseases of the parotid gland.
Conclusion The proposed localization landmarks allowed a fast and safe identification of the facial nerve and may be of significant help during surgery around the parotid region. Reasonable speed and safety in identifying and preserving important anatomical structures are of vital importance for successful surgery in all specialties.
Furthermore, in circumstances where reoperation is required, the usual surgical landmarks for the facial nerve main trunk become useless, because scar tissue, inflammation, or even recurrent disease may have distorted the surgical field .
Clinical Anatomy Page 1 of 9 F : Davies JC, Agur AMR, Fattah AY i r r ii e re e i O O A } v ] µ } v A A Y AY Z ] ere e : ieee uiig rei e riui iee æ Review Abstract Introduction Facial nerve injury may have devas-tating effects on function, aesthetics and the social interaction of the affected patients. Much energy has been devoted to reliably determining landmarks to predict the course of
Cosmetic Surgical Anatomy of the Ligamentous Attachments
8/02/2016 · The surgical anatomy and landmarks of the facial nerve. View Media Gallery. Surgical landmarks to the facial nerve include the tympanomastoid suture line, the tragal pointer, and the posterior belly of the digastric muscle. The tympanomastoid suture line lies between the mastoid and tympanic segments of the temporal bone and is approximately 6-8 mm lateral to the stylomastoid …
This study describes the microsurgical anatomy of the middle cranial fossa approach using temporal bone three-dimensional (3D) computed tomography (CT) reconstruction, which should contribute to determining the drilling point for the internal auditory meatus (IAM) when bony landmarks are absent
landmarks including the mastoid pro-cess, posterior belly of digastric muscle, The surgical pro-cedure was initiated using a modified Blair incision, raising the sub-superficial musculoaponeurotic system, sub-platysmal flap until we reached the masseter muscle. The aim was to identify the FN using an antegrade technique. To achieve this aim, the greater auricular nerve was identified and
TRAGAL POINTER AS A SURGICAL LANDMARK FOR THE IDENTIFICATION OF FACIAL NERVE TRUNK IN PAROTIDECTOMY: OUR EXPERIENCE Ihsanullah, Sharafat Ali …
Until recently, tympanic facial nerve surgery had been performed using microscopic approaches, but in recent years, exclusive endoscopic approaches to the middle ear have increasingly been used, particularly in cholesteatoma surgery.
surgical landmarks for avoiding injury to the facial nerve and advocated complete removal of the superficial portion of the parotid gland for noninvasive lesions confined to that portion of the gland11. This concept was improved upon and has resulted in a refinement of parotid surgery to include the following principles: Firstly, the parotid tumour should be more aggressively removed with an
Many surgical landmarks have been suggested to help the surgeon identify the facial nerve when performing parotid gland surgery. There is no conclusive evidence that any one landmark is better than the rest. In this study distances from the most frequently used surgical landmarks to the main trunk of the facial nerve were measured in 30 halves of cadaver heads. Two ENT surgeons assessed the
facial paralysis (3 weeks to 2 yr) and chronic facial paralysis (>2 yr). For acute facial paralysis, the main surgical therapies For acute facial paralysis, the main surgical therapies are facial nerve decompression and facial nerve repair.
plastic surgery center, ny ximena wortsman, md radiologist santiago, chile . imaging parameters linear array 14-18 mhz 3d array 15-17 mhz with surface rendering display linear electronic array 20-40 mhz doppler color, power, spectral with vessel density histogram analysis . facial nerve imaging superficial facial nerves are difficult to image in standard cross sections 3d representation of a
A number of different approaches can be used to expose the facial nerve. The route taken will depend on the pathology and the portion of the nerve that requires exposure. When performing a
Applied Surgical anatomy of Facial Nerve in Oral & Maxillofacial Surgery Damage to facial nerve is possible in severe maxillofacial surgeries with basilar skull fractures anywhere in the area of course of the nerve and would result in ipsilateral paralysis of the muscles of facial expression Of concern to the surgeon is the close proximity of the main trunk of facial nerve where it exits the
facial nerve and the facial artery and vein. There is a specific anatomic relationship between There is a specific anatomic relationship between these structures that is discussed later.
TRAGAL POINTER AS A SURGICAL LANDMARK FOR THE
Facial nerve Wikipedia
Surgical Anatomy of the Mandibular Region for
Landmarks for parotid gland surgery cambridge.org
https://youtube.com/watch?v=kvmwsTU0InQ
Parotid Gland Surgery for Benign Tumours Have We Come
Facial nerve Wikipedia
Anatomy of Meckel’s Cave and the Trigeminal ganglion
Various surgical landmarks of the facial nerve have been investigated to allow for a safer and quicker parotidectomy or other surgery in the lateral face. Surface landmarks for the facial nerve trunk have been proposed. Pather and Osman [14] suggested the use of the transverse process of the axis as the landmark for the facial nerve trunk because it was easily palpated, did not require a
Marginal mandibular branch of facial nerve Mid-inguinal point – half way between ASIS and pubis – landmark for femoral artery in groin. (see lower limb pulses and cardiovascular examination). 18. Midpoint of inguinal ligament – Half way between ASIS and pubic tubercle – landmark for deep inguinal ring and indirect inguinal hernia. Medial to this for direct inguinal hernia. 19. Inguinal
Facial nerve paralysis is a daunting potential complication of parotid surgery and is widely reported. Knowledge of the key landmarks of the facial nerve trunk is essential for safe and effective
surgery is between 3% and 5% and that of postoperative transient facial nerve dysfunction, between 8.2% and 65% (Witt, 1998). During parotid gland surgery, preservation of the facial
facial nerve and the facial artery and vein. There is a specific anatomic relationship between There is a specific anatomic relationship between these structures that is discussed later.
facial skin and Superficial Muscular Aponeurotic System (SMAS) during facial rejuvenation procedures. The aim of this study was to The aim of this study was to define the location of the true retaining ligaments of the face and to discuss their usability as surgical landmarks.
ultrasound anatomy of the facial danger zones robert bard, md director, the biofoundation for angiogenesis research, ny j. pozner, md & l. bass, md plastic surgery center, ny ximena wortsman, md radiologist santiago, chile . imaging parameters linear array 14-18 mhz 3d array 15-17 mhz with surface rendering display linear electronic array 20-40 mhz doppler color, power, spectral with vessel
Facial nerve trunk variations with surgical implications
A review of the tragal pointer anatomy and its importance
surgical landmarks for avoiding injury to the facial nerve and advocated complete removal of the superficial portion of the parotid gland for noninvasive lesions confined to that portion of the gland11. This concept was improved upon and has resulted in a refinement of parotid surgery to include the following principles: Firstly, the parotid tumour should be more aggressively removed with an
skeletonization of the facial nerve along the mastoid segment to lower the posterior canal wall to the facial nerve (still covered by bone). The mastoid area behind the facial nerve is later obliterated with a muscle flap to keep the volume of the final cavity low and avoid discharging ears. The other method of “canal wall down” mastoidectomy is front-to-back mastoidec-tomy. Surgeons may
Conclusion The proposed localization landmarks allowed a fast and safe identification of the facial nerve and may be of significant help during surgery around the parotid region. Reasonable speed and safety in identifying and preserving important anatomical structures are of vital importance for successful surgery in all specialties.
In this particular case, the knowledge of surgical anatomy of the facial nerve and its correlations with the parotid gland is very important for an adequate preservation in the cases of surgery of benign and malignant diseases of the parotid gland.
Background: The identification of the facial nerve can be difficult in a bloody operative field or by an incision that limits exposure; hence anatomic al landmarks and adequate operative exposure can aid such identification and preservation.
Penetration of the parotid gland near the facial nerve has always raised concerns among surgeons because facial nerve injury is an important cause of morbidity associated with parotid gland surgery. The conventional approach is anterograde parotidectomy, in which the main trunk of the facial nerve (facial nerve trunk, FNT) is identified and
variations of the tympanomastoid segment of the facial nerve in relation to fixed known anatomical landmarks in cadaveric temporal bone dissection. 395 . 396 Safer Ear Surgery: Anatomical Study of Landmarks Materials and Methods 35 human temporal bones (18 right and 17 left) were obtained and dissected with standard otologic instruments under magnification using Karl Kaps (Germany) …
Facial Nerve Parotid Landmark – Free download as PDF File (.pdf), Text File (.txt) or read online for free. Landmarks of the Facial Nerve as it leaves the Parotid Landmarks of the Facial Nerve as it leaves the Parotid
Anatomy of the facial nerve branching patterns the
Facial nerve ppt roger original slideshare.net
In our study, the facial nerve was an average of 5.22 mm from the petrous ridge. The longest distance was 10.1 mm. When drilling at the The longest distance was 10.1 mm. When drilling at the internal acoustic opening of the IAM, one should be cautious until the facial nerve is found.
distance from the arcuate eminence, the facial nerve hiatus, and the foramen spinosum to MC was 16.6, 12.8 and 7.46 mm respectively. The TG The TG lay 5.81 mm posterior to the foramen ovale.
Facial nerve injury during rhytidectomy is a rare but dreaded complication. Of the various divisions of the facial nerve, injury to the marginal mandibular nerve (MMN) is of great concern in planning for a lower face- or necklift.
Clinical Anatomy Page 1 of 9 F : Davies JC, Agur AMR, Fattah AY i r r ii e re e i O O A } v ] µ } v A A Y AY Z ] ere e : ieee uiig rei e riui iee æ Review Abstract Introduction Facial nerve injury may have devas-tating effects on function, aesthetics and the social interaction of the affected patients. Much energy has been devoted to reliably determining landmarks to predict the course of
Background. The identification of the facial nerve can be difficult in a bloody operative field or by an incision that limits exposure; hence anatomical landmarks and adequate operative exposure can aid such identification and preservation.
facial nerve trunk was 3.5 mm (cadaver) and 3.87 mm (live surgery), the tragal pointer was found to be at a mean distance of 16.61 mm (cadaver) and 16.36 mm (live sur-
This study describes the microsurgical anatomy of the middle cranial fossa approach using temporal bone three-dimensional (3D) computed tomography (CT) reconstruction, which should contribute to determining the drilling point for the internal auditory meatus (IAM) when bony landmarks are absent
facial nerve and the facial artery and vein. There is a specific anatomic relationship between There is a specific anatomic relationship between these structures that is discussed later.
– Facial nerve – Facial retaining ligaments Techniques – SMAS lift – Deep-plane lift – Composite lift – Subperiosteal lift Nasolabial fold Non-surgical facelift . Anatomy Platysma muscle – from the lower cheek to the level of the second rib – Three variations of the anterior boarders of the right and left platysma muscle Type1: separated in the suprahyoid region and interlacing
Facial nerve is the seventh cranial nerve, which supplies the muscles of the facial expression, sensory supply to the an- terior two thirds of the tongue and secretomotor supply to
Conclusion The proposed localization landmarks allowed a fast and safe identification of the facial nerve and may be of significant help during surgery around the parotid region. Reasonable speed and safety in identifying and preserving important anatomical structures are of vital importance for successful surgery in all specialties.
⭐⭐⭐The tympanomastoid suture line⭐⭐⭐ ⭐⭐⭐The posterior digastric muscle⭐⭐⭐ The tragal pointer refers to the tragus cartilage, which “points” to the location of the nerve one centimeter anterior, inferior, and deep to the cartilage.
Local Anesthesia Techniques in Oral and Maxillofacial Surgery Sean M. Healy, D.D.S. Oral and Maxillofacial Surgery Francis B. Quinn, M.D., FACS
Division of Plastic and Reconstructive Surgery, Washington University School of Medicine, Suite 17424, East Pavilion, Box 8238, One Barnes-Jewish Hospital Plaza, Saint Louis, MO 63110, USA. Treatment of facial nerve injuries depends upon a detailed understanding of its anatomic course, accurate clinical examination, and timely and appropriate diagnostic studies.
A review of the tragal pointer: anatomy and its importance as a landmark in surgical procedures llary artery to the tragal pointer, Frankfort hori- zontal plane, and tip of the condyle (Table 3).
Surgical landmarks for identification of facial nerve in
Rhytidectomy University of Texas Medical Branch
surgery is between 3% and 5% and that of postoperative transient facial nerve dysfunction, between 8.2% and 65% (Witt, 1998). During parotid gland surgery, preservation of the facial
A number of different approaches can be used to expose the facial nerve. The route taken will depend on the pathology and the portion of the nerve that requires exposure. When performing a
facial paralysis (3 weeks to 2 yr) and chronic facial paralysis (>2 yr). For acute facial paralysis, the main surgical therapies For acute facial paralysis, the main surgical therapies are facial nerve decompression and facial nerve repair.
24/07/2013 · Aims and Objectives. The aim of the cadaveric dissection was to dissect all the landmarks of facial nerve that has been described in the literature and study their respective anatomical relationship with the facial nerve.
TRAGAL POINTER AS A SURGICAL LANDMARK FOR THE IDENTIFICATION OF FACIAL NERVE TRUNK IN PAROTIDECTOMY: OUR EXPERIENCE Ihsanullah, Sharafat Ali …
Facial nerve paralysis is a daunting potential complication of parotid surgery and is widely reported. Knowledge of the key landmarks of the facial nerve trunk is essential for safe and effective
landmarks including the mastoid pro-cess, posterior belly of digastric muscle, The surgical pro-cedure was initiated using a modified Blair incision, raising the sub-superficial musculoaponeurotic system, sub-platysmal flap until we reached the masseter muscle. The aim was to identify the FN using an antegrade technique. To achieve this aim, the greater auricular nerve was identified and
Injury to the marginal mandibular branch of the facial nerve (MMN) during surgery often results in poor functional and cosmetic outcomes. A line two finger breadths or 2 cm inferior to the border of the mandible is commonly used in planning neck incisions to avoid injury to the MMN. The purpose was to compare the two finger breadth/2 cm landmarks in predicting MMN course, and their accuracy
facial skin and Superficial Muscular Aponeurotic System (SMAS) during facial rejuvenation procedures. The aim of this study was to The aim of this study was to define the location of the true retaining ligaments of the face and to discuss their usability as surgical landmarks.
The facial nerve is the seventh cranial nerve, or simply CN VII. It emerges from the pons of the brainstem, controls the muscles of facial expression, and functions in the conveyance of taste sensations from the anterior two-thirds of the tongue. The nerves typically travels from the pons through the facial canal in the temporal bone and exits the skull at the stylomastoid foramen. It arises
A cadaveric study of surgical landmarks for retrograde
Anatomy of the Facial Nerve and its Implication in the
Conclusion The proposed localization landmarks allowed a fast and safe identification of the facial nerve and may be of significant help during surgery around the parotid region. Reasonable speed and safety in identifying and preserving important anatomical structures are of vital importance for successful surgery in all specialties.
of information on the deep attachments in the cheek.18,21 Recently, studies have begun to in-vestigate deep attachments found in the tem-poral12,25 and periorbital regions.26,27 These ar-
Until recently, tympanic facial nerve surgery had been performed using microscopic approaches, but in recent years, exclusive endoscopic approaches to the middle ear have increasingly been used, particularly in cholesteatoma surgery.
Background: The identification of the facial nerve can be difficult in a bloody operative field or by an incision that limits exposure; hence anatomic al landmarks and adequate operative exposure can aid such identification and preservation.
Facial nerve paralysis is a daunting potential complication of parotid surgery and is widely reported. Knowledge of the key landmarks of the facial nerve trunk is essential for safe and effective
described the facial nerve line, which extends from the lateral surface of the posterior belly of the digastric muscle to the lateral surface of the ascending ramus. 2 The spatial relation-
facial nerve and the facial artery and vein. There is a specific anatomic relationship between There is a specific anatomic relationship between these structures that is discussed later.
N. Pather Landmarks of the facial nerve implications for
A cadaveric study of surgical landmarks for retrograde
A number of different approaches can be used to expose the facial nerve. The route taken will depend on the pathology and the portion of the nerve that requires exposure. When performing a
Facial nerve is the seventh cranial nerve, which supplies the muscles of the facial expression, sensory supply to the an- terior two thirds of the tongue and secretomotor supply to
21/07/2015 · The facial nerve, or cranial nerve (CN) VII, is the nerve of facial expression. The pathways of the facial nerve are variable, and knowledge of the key intratemporal and extratemporal landmarks is essential for accurate physical diagnosis and safe and effective surgical intervention in …
distance from the arcuate eminence, the facial nerve hiatus, and the foramen spinosum to MC was 16.6, 12.8 and 7.46 mm respectively. The TG The TG lay 5.81 mm posterior to the foramen ovale.
Errors in facial nerve surgery 319 An example is that of playing chess. A novice may have only a handful of memorized defense strategies.
facial skin and Superficial Muscular Aponeurotic System (SMAS) during facial rejuvenation procedures. The aim of this study was to The aim of this study was to define the location of the true retaining ligaments of the face and to discuss their usability as surgical landmarks.
The facial nerve is the seventh cranial nerve, or simply CN VII. It emerges from the pons of the brainstem, controls the muscles of facial expression, and functions in the conveyance of taste sensations from the anterior two-thirds of the tongue. The nerves typically travels from the pons through the facial canal in the temporal bone and exits the skull at the stylomastoid foramen. It arises
Facial nerve paralysis is a daunting potential complication of parotid surgery and is widely reported. Knowledge of the key landmarks of the facial nerve trunk is essential for safe and effective
skeletonization of the facial nerve along the mastoid segment to lower the posterior canal wall to the facial nerve (still covered by bone). The mastoid area behind the facial nerve is later obliterated with a muscle flap to keep the volume of the final cavity low and avoid discharging ears. The other method of “canal wall down” mastoidectomy is front-to-back mastoidec-tomy. Surgeons may
Identification of the facial nerve trunk is essential during surgery of the parotid gland. Numerous landmarks have been researched and used. The relation between the facial nerve to two constant bony landmarks, the tip of the mastoid process and the central point of the transverse process of the atlas was investigated.
well-defined surgical landmarks, and not at least, the personal experience of the surgeon in this type of surgery. The main roles of monitoring the facial nerve are: reducing the risck of iatrogenic trauma during dissection, mapping the course of the nerve, early nerve identification and warning the surgeon about the proximity of the nerve during dissection (18). Usually there are four
Critical surgical landmarks for this procedure are the digastric ridge (i.e. a ridge of bone, which is posterior to the facial nerve and medial to the tip of the mastoid), the fossa incudis and
IrJNS. 2017;2(4) 77. surgical landmarks to perform a safe surgery [11]. Due to the stressful nature of the surgery and possible facial nerve injury and so many problems of facial nerve and subsequent
described the facial nerve line, which extends from the lateral surface of the posterior belly of the digastric muscle to the lateral surface of the ascending ramus. 2 The spatial relation-
Local Anesthesia Techniques in Oral and Maxillofacial Surgery Sean M. Healy, D.D.S. Oral and Maxillofacial Surgery Francis B. Quinn, M.D., FACS
Identifying a Safe Zone for Midface Augmentation Using
Evaluation of Two Facial Nerve Landmarks Frequency in
Although the surgical anatomy of the facial nerve has been well documented, the concept of surgical treatment for parotid tumors, facial palsy (neurorraphy techniques) and submandibular surgical approach are rarely challenged now.
TRAGAL POINTER AS A SURGICAL LANDMARK FOR THE IDENTIFICATION OF FACIAL NERVE TRUNK IN PAROTIDECTOMY: OUR EXPERIENCE Ihsanullah, Sharafat Ali …
variations of the tympanomastoid segment of the facial nerve in relation to fixed known anatomical landmarks in cadaveric temporal bone dissection. 395 . 396 Safer Ear Surgery: Anatomical Study of Landmarks Materials and Methods 35 human temporal bones (18 right and 17 left) were obtained and dissected with standard otologic instruments under magnification using Karl Kaps (Germany) …
Abstract. Facial nerve paralysis is a daunting potential complication of parotid surgery and is widely reported. Knowledge of the key landmarks of the facial nerve trunk is essential for safe and effective surgical intervention in the region of the parotid gland.
Conclusion The proposed localization landmarks allowed a fast and safe identification of the facial nerve and may be of significant help during surgery around the parotid region. Reasonable speed and safety in identifying and preserving important anatomical structures are of vital importance for successful surgery in all specialties.
– Facial nerve – Facial retaining ligaments Techniques – SMAS lift – Deep-plane lift – Composite lift – Subperiosteal lift Nasolabial fold Non-surgical facelift . Anatomy Platysma muscle – from the lower cheek to the level of the second rib – Three variations of the anterior boarders of the right and left platysma muscle Type1: separated in the suprahyoid region and interlacing
8/02/2016 · The surgical anatomy and landmarks of the facial nerve. View Media Gallery. Surgical landmarks to the facial nerve include the tympanomastoid suture line, the tragal pointer, and the posterior belly of the digastric muscle. The tympanomastoid suture line lies between the mastoid and tympanic segments of the temporal bone and is approximately 6-8 mm lateral to the stylomastoid …
Facial nerve paralysis is a daunting potential complication of parotid surgery and is widely reported. Knowledge of the key landmarks of the facial nerve trunk is essential for safe and effective
A number of different approaches can be used to expose the facial nerve. The route taken will depend on the pathology and the portion of the nerve that requires exposure. When performing a
facial nerve trunk was 3.5 mm (cadaver) and 3.87 mm (live surgery), the tragal pointer was found to be at a mean distance of 16.61 mm (cadaver) and 16.36 mm (live sur-
Original Article Surgical Dissection of the Facial nerve in Parotidectomy: Our Personal Experience *Nematollah Mokhtari Amir Majdi1, Mojgan Pourhamzeh2 Abstract Introduction: Salivary gland tumors are relatively rare and constitute 3-4% of all head and neck neoplasms. The majority (70%) of salivary gland tumors arise in the parotid gland. Recommended treatment for a parotid mass is surgical
Anatomy of Meckel’s Cave and the Trigeminal ganglion
The surgical management of facial nerve injury. PubFacts
facial skin and Superficial Muscular Aponeurotic System (SMAS) during facial rejuvenation procedures. The aim of this study was to The aim of this study was to define the location of the true retaining ligaments of the face and to discuss their usability as surgical landmarks.
21/07/2015 · The facial nerve, or cranial nerve (CN) VII, is the nerve of facial expression. The pathways of the facial nerve are variable, and knowledge of the key intratemporal and extratemporal landmarks is essential for accurate physical diagnosis and safe and effective surgical intervention in …
variations of the tympanomastoid segment of the facial nerve in relation to fixed known anatomical landmarks in cadaveric temporal bone dissection. 395 . 396 Safer Ear Surgery: Anatomical Study of Landmarks Materials and Methods 35 human temporal bones (18 right and 17 left) were obtained and dissected with standard otologic instruments under magnification using Karl Kaps (Germany) …
Facial nerve injury during rhytidectomy is a rare but dreaded complication. Of the various divisions of the facial nerve, injury to the marginal mandibular nerve (MMN) is of great concern in planning for a lower face- or necklift.
Critical surgical landmarks for this procedure are the digastric ridge (i.e. a ridge of bone, which is posterior to the facial nerve and medial to the tip of the mastoid), the fossa incudis and
The facial nerve is the seventh cranial nerve, or simply CN VII. It emerges from the pons of the brainstem, controls the muscles of facial expression, and functions in the conveyance of taste sensations from the anterior two-thirds of the tongue. The nerves typically travels from the pons through the facial canal in the temporal bone and exits the skull at the stylomastoid foramen. It arises
Identifying a Safe Zone for Midface Augmentation Using
Landmarks for parotid gland surgery cambridge.org
landmarks including the mastoid pro-cess, posterior belly of digastric muscle, The surgical pro-cedure was initiated using a modified Blair incision, raising the sub-superficial musculoaponeurotic system, sub-platysmal flap until we reached the masseter muscle. The aim was to identify the FN using an antegrade technique. To achieve this aim, the greater auricular nerve was identified and
facial nerve is not a true anatomic separation into two distinct and discrete lobes.1 During parotidectomy, several anatomical landmarks may be used to locate the facial nerve. One of the most commonly employed is the tragal pointer.
Applied Surgical anatomy of Facial Nerve in Oral & Maxillofacial Surgery Damage to facial nerve is possible in severe maxillofacial surgeries with basilar skull fractures anywhere in the area of course of the nerve and would result in ipsilateral paralysis of the muscles of facial expression Of concern to the surgeon is the close proximity of the main trunk of facial nerve where it exits the
Facial nerve paralysis is a daunting potential complication of parotid surgery and is widely reported. Knowledge of the key landmarks of the facial nerve trunk is essential for safe and effective surgical intervention in the region of the parotid
Identification of the facial nerve trunk is essential during surgery of the parotid gland. Numerous landmarks have been researched and used. The relation between the facial nerve to two constant bony landmarks, the tip of the mastoid process and the central point of the transverse process of the atlas was investigated.
Surgical exposure of the facial nerve.11 Learning to use this landmark requires more surgical expertise and does not predict more accurately the position of the facial nerve trunk than other methods reported. Acta Otolaryngol Suppl. 13. 4.80:261-273.40 (0.03.
Daniel Jose C. Mendoza MD Intraoperative Distance Between
Identification of Facial Nerve During Parotidectomy A
facial paralysis (3 weeks to 2 yr) and chronic facial paralysis (>2 yr). For acute facial paralysis, the main surgical therapies For acute facial paralysis, the main surgical therapies are facial nerve decompression and facial nerve repair.
21/07/2015 · The facial nerve, or cranial nerve (CN) VII, is the nerve of facial expression. The pathways of the facial nerve are variable, and knowledge of the key intratemporal and extratemporal landmarks is essential for accurate physical diagnosis and safe and effective surgical intervention in …
Local Anesthesia Techniques in Oral and Maxillofacial Surgery Sean M. Healy, D.D.S. Oral and Maxillofacial Surgery Francis B. Quinn, M.D., FACS
Facial nerve paralysis is a daunting potential complication of parotid surgery and is widely reported. Knowledge of the key landmarks of the facial nerve trunk is essential for safe and effective surgical intervention in the region of the parotid
Many surgical landmarks have been suggested to help the surgeon identify the facial nerve when performing parotid gland surgery. There is no conclusive evidence that any one landmark is better than the rest. In this study distances from the most frequently used surgical landmarks to the main trunk of the facial nerve were measured in 30 halves of cadaver heads. Two ENT surgeons assessed the
– Facial nerve – Facial retaining ligaments Techniques – SMAS lift – Deep-plane lift – Composite lift – Subperiosteal lift Nasolabial fold Non-surgical facelift . Anatomy Platysma muscle – from the lower cheek to the level of the second rib – Three variations of the anterior boarders of the right and left platysma muscle Type1: separated in the suprahyoid region and interlacing
Facial nerve Wikipedia
Daniel Jose C. Mendoza MD Intraoperative Distance Between
Facial nerve paralysis is a daunting potential complication of parotid surgery and is widely reported. Knowledge of the key landmarks of the facial nerve trunk is essential for safe and effective surgical intervention in the region of the parotid gland.
Background. The identification of the facial nerve can be difficult in a bloody operative field or by an incision that limits exposure; hence anatomical landmarks and adequate operative exposure can aid such identification and preservation.
Various surgical landmarks of the facial nerve have been investigated to allow for a safer and quicker parotidectomy or other surgery in the lateral face. Surface landmarks for the facial nerve trunk have been proposed. Pather and Osman [14] suggested the use of the transverse process of the axis as the landmark for the facial nerve trunk because it was easily palpated, did not require a
IrJNS. 2017;2(4) 77. surgical landmarks to perform a safe surgery [11]. Due to the stressful nature of the surgery and possible facial nerve injury and so many problems of facial nerve and subsequent
facial skin and Superficial Muscular Aponeurotic System (SMAS) during facial rejuvenation procedures. The aim of this study was to The aim of this study was to define the location of the true retaining ligaments of the face and to discuss their usability as surgical landmarks.
described the facial nerve line, which extends from the lateral surface of the posterior belly of the digastric muscle to the lateral surface of the ascending ramus. 2 The spatial relation-
Landmarks used to localise the marginal mandibular branch of the facial nerve (MMN) included: the angle of the mandible, facial artery, inferior border of mandible, parotid edge, lobule, gonion, retromandibular vein and massteric tuberosity of the mandible [21,22,23,24].
Identifying Facial Nerve Surgery Anatomy Scribd
What are landmarks used to find the facial nerve during
8/02/2016 · The surgical anatomy and landmarks of the facial nerve. View Media Gallery. Surgical landmarks to the facial nerve include the tympanomastoid suture line, the tragal pointer, and the posterior belly of the digastric muscle. The tympanomastoid suture line lies between the mastoid and tympanic segments of the temporal bone and is approximately 6-8 mm lateral to the stylomastoid …
21/07/2015 · The facial nerve, or cranial nerve (CN) VII, is the nerve of facial expression. The pathways of the facial nerve are variable, and knowledge of the key intratemporal and extratemporal landmarks is essential for accurate physical diagnosis and safe and effective surgical intervention in …
Penetration of the parotid gland near the facial nerve has always raised concerns among surgeons because facial nerve injury is an important cause of morbidity associated with parotid gland surgery. The conventional approach is anterograde parotidectomy, in which the main trunk of the facial nerve (facial nerve trunk, FNT) is identified and
facial nerve trunk was 3.5 mm (cadaver) and 3.87 mm (live surgery), the tragal pointer was found to be at a mean distance of 16.61 mm (cadaver) and 16.36 mm (live sur-
Original Article Surgical Dissection of the Facial nerve in Parotidectomy: Our Personal Experience *Nematollah Mokhtari Amir Majdi1, Mojgan Pourhamzeh2 Abstract Introduction: Salivary gland tumors are relatively rare and constitute 3-4% of all head and neck neoplasms. The majority (70%) of salivary gland tumors arise in the parotid gland. Recommended treatment for a parotid mass is surgical
Three-dimensional Anatomical Analysis of Surgical
Facial nerve trunk variations with surgical implications
This study describes the microsurgical anatomy of the middle cranial fossa approach using temporal bone three-dimensional (3D) computed tomography (CT) reconstruction, which should contribute to determining the drilling point for the internal auditory meatus (IAM) when bony landmarks are absent
Many surgical landmarks have been suggested to help the surgeon identify the facial nerve when performing parotid gland surgery. There is no conclusive evidence that any one landmark is better than the rest. In this study distances from the most frequently used surgical landmarks to the main trunk of the facial nerve were measured in 30 halves of cadaver heads. Two ENT surgeons assessed the
landmarks including the mastoid pro-cess, posterior belly of digastric muscle, The surgical pro-cedure was initiated using a modified Blair incision, raising the sub-superficial musculoaponeurotic system, sub-platysmal flap until we reached the masseter muscle. The aim was to identify the FN using an antegrade technique. To achieve this aim, the greater auricular nerve was identified and
distance from the arcuate eminence, the facial nerve hiatus, and the foramen spinosum to MC was 16.6, 12.8 and 7.46 mm respectively. The TG The TG lay 5.81 mm posterior to the foramen ovale.
Background The identification of the facial nerve can be difficult in a bloody operative field or by an incision that limits exposure; hence anatomical landmarks and adequate operative exposure can aid such identification and preservation. In this
Clinical Anatomy Page 1 of 9 F : Davies JC, Agur AMR, Fattah AY i r r ii e re e i O O A } v ] µ } v A A Y AY Z ] ere e : ieee uiig rei e riui iee æ Review Abstract Introduction Facial nerve injury may have devas-tating effects on function, aesthetics and the social interaction of the affected patients. Much energy has been devoted to reliably determining landmarks to predict the course of
Surgical Management of Iatrogenic Facial Nerve Injuries
A review of the tragal pointer anatomy and its importance
World Journal of Surgical Oncology BioMed Central